Endodontists always strive to get to the root of the problem. Since the areas of most concern for our specialty are often indiscernible, even on an x-ray, cone-beam CT imaging offers endodontists a non-distorted, cross-sectional view of the mouth that uncovers many vital issues that affect the direction of our treatment.
The 3D capability of the scan allows us to rotate and see dental structures from different angles, giving new perspective and many times averting unnecessary or premature procedures. 3D radiography can be immensely valuable in detecting and assessing resorption, re-treatment, small cracks, hidden canals, foreign bodies, the extent of decay to the crestal bone, and hidden infections.
Since having the most accurate information possible facilitates the most defined treatment, details are central to any dentist's diagnosis. However, endodontists in particular can benefit from the gamut of cone beam's imaging capabilities.
Minute details
For example, patients often arrive at our office with symptoms ranging from "I’m not sure which tooth hurts" to excruciating pain, with other vague descriptions that make an accurate diagnosis difficult without exploratory surgery. A 3D image often can provide the minute details that pinpoint the problematic areas. I have witnessed patients complaining of tenderness from infections that were too small to discern on X-rays that showed up on a 3D scan, as well as infections draining into the sinus that could have caused complications if left untreated before further procedures were before.
 |
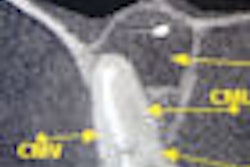
| The power of 3D cross-sections |
With the different cone-beam CT machines and fields-of -view available, dentists can determine which machine is most appropriate for their practice. A cone beam system with a small field-of-view is especially helpful when viewing one to three teeth maximum. The quality of the images with this machine is beneficial in diagnosing single problematic areas, particularly in resorption defects, fractures, and retreatment cases.
An advantage to large fields of view would be to determine symmetry. Occasionally there will be a lesion present and the need for a scan on the opposite arch is helpful in determining if it is normal. Also when there are difficult teeth to treat, a full scan of one arch can be helpful in determining whether extra canals are truly evident. For example, a retreatment case that is difficult to determine if a 2nd, 3rd, or 4th canal is present due to the prior treatment can also be viewed with its counterpart. If a canal is demonstrated in its counterpart, there will surely be one in the case in question.
 |
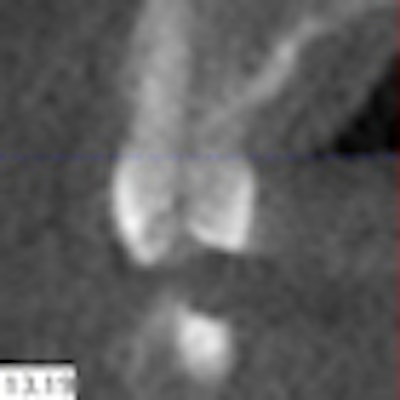
| Cone beam CT images can provide axial views not possible with traditional 2D imaging. |
Also with a single-arch scan, sinus infections or abnormal sinuses can be shown to the patient. For example, a patient who has had an infection in the upper first molar had complications with the sinus that was easily detected with a 4 cm single-arch scan. By viewing the opposite side, the sinuses were clear in one side while the arch in question had some type of irritation present in it. Also with a full-arch scan, another patient had a break in the sinus and the infection was draining right into it.
Note that single-arch scans are not full upper- and lower-arch scans. Full upper- and lower-arch scans can be done, however, enabling easy diagnosis of the entire mouth. For example, we took a full upper and lower arch scan and determined other pathology not noted from the referring dentist or from regular bitewing checkups.
Pre-treatment and re-treatment
As an endodontist, I appreciate the pre-surgery view that a cone beam image supplies. Before 3D scans were a convenient in-office option, information on conditions that lurked under the gum would require an invasive procedure involving numbing the patient and incising and flapping the gum. A cone beam scan is a much less stressful option than exploratory gum surgery.
Besides pre-treatment, 3D scans also help to prevent unnecessary re-treatment. With the ability to detect small cracks provided by cone-beam scans, we can avoid the guesswork of performing certain procedures, only to have to "try again" when the symptoms fail to clear up. The same is true for resorption. While apical resorption is somewhat possible to detect on a typical radiograph, assessing the buccal and lingual areas can be somewhat more evasive. With a 3D view, I can visualize the teeth relative to other anatomical structures or see how deeply decay has moved into the gum or bone.
Cone-beam scans also offer precise images of anatomical parts that are central to root-canal procedures, root location, thickness of bone, and the placement of roots in relation to the surrounding jaw. Anatomical structures such as the maxillary sinus and dental nerves and root apices are also clearly defined.
Dentists can also adjust the resolution to suit each individual case. While high-resolution scans are best for endodontics, it is not necessary at all times. By looking at the cross sections of teeth and measurements, we can sometime determine the problem without using high resolution. In my office, we often take scans at either 0.12 or 0.4 resolution, even on occasion half scans.
Patient and doctor education
Detecting conditions early, before larger problems evolve, makes our job easier and also builds patient confidence. To visualize their tooth in its entirety is a loyalty builder. As I continue to discover with my cone-beam CT system, when we can tell our patients that they may not require surgery because we employ the latest technology, the good news will spread to their friends and family. Besides just telling our patients what we can do for them, they can view detailed scans with us in the office at the first visit. They will be more apt to understand and accept treatment. I don't know of anyone who would choose exploratory surgery over a quick cone-beam scan, conveniently located in my office.
To reap the most benefits out of our cone-beam systems, dental professionals must continually keep learning about cone beam imaging and its capabilities. Attending seminars on training and implementation of the new technology can improve our methods and our practice-s profitability. As endodontists, we should strive to uncover as many of the facts as we can with our imaging options.
Currently, cone beam CT is utilized as an addition to our primary imaging methods; however, I believe that the scans will become the standard of care. We currently utilize scans with the GX CB-500 (Gendex Dental Systems) as our standard. We have made a decision to scan all upper molar cases as well as retreatment cases, all apical surgeries, and any other teeth that are deemed questionable. The scans provide a more thorough and accurate diagnosis as well as aiding in the procedure to help save teeth that may otherwise have been deemed non-restorable. The images also educate the patients and give them an opportunity to have a role in the treatment plan with the doctors. Knowing what truly lies beneath the surface is good for patients and doctors, as well as their practices.
Ralan Wong, D.D.S., M.S., is associate clinical professor in endodontics at the University of the Pacific School of Dentistry. He graduated with honors from the University of the Pacific College in 1989 and the School of Dentistry in 1992. He completed his graduate training in endodontics at the University of Pennsylvania School of Dental Medicine in 1997.