Do panoramic bitewings offer enough advantages over intraoral bitewings to warrant using this extraoral method rather than the traditional approach? Some manufacturers and clinicians contend they do, but others say more peer-reviewed research is needed.
"Traditionally, dentists have believed that the resolution of panoramic x-rays and the ability to open the contacts were not as good as with traditional bitewings," wrote Robert Langlais, DDS, MS, a professor at the University of Texas Health Science Center at San Antonio, earlier this year in Dental Economics. However, he noted, "recent research ... has determined how to open the posterior contacts to get a panoramic bitewing" (Dentomaxillofacial Radiology, January 2010, Vol. 39:1, pp. 47-53).
He goes on to list six reasons why dental practitioners should consider using a panoramic x-ray system for bitewings:
- Better patient acceptance
- Easier for the dentist and staff
- Faster
- More diagnostic
- Less radiation exposure
- Better infection control
"There are literally no downsides to this," said Jim Hooper, the district sales manager for Planmeca, which markets its Promax system for this application and has sold more than 300 systems in the past two years specially for pano bitewings. "There is less radiation to the patient; if you use round collimation and D-speed film, four bitewings have five times the dose of one pano. Also, it takes less time; it can take five minutes or more to take an intraoral bitewing series."
In addition, he noted, by using the Promax to take bitewings, the practitioner is able to see the apices and do more dentistry, "because you are basically taking a full-mouth series with the pan."
 |
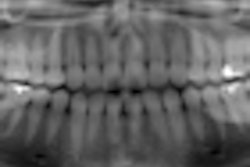
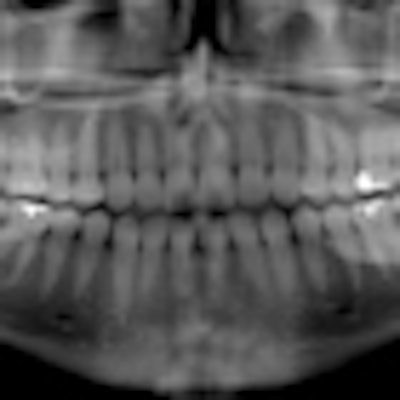
| Click here to enlarge this image. |
| These panoramic bitewings took 15 to 20 seconds to create, compared with 20 minutes for a full-mouth intraoral survey (Dentomaxillofacial Radiology, January 2010, Vol. 39:1, pp. 47-53). |
From the patient's perspective, "there isn't one patient alive who says they enjoy the sensor experience," Hooper said. "So if you give them the choice of standing there and biting on a bite stick while the pan goes around their head, versus chomping on a sensor four times, they will pick the pano every time."
The only potential downside is related to positioning, he acknowledged. "If you do the positioning poorly, you won't get open contacts," he said.
The Promax opens contacts at least as consistently, "if not more so," than any intraoral modality except maybe film, Hooper added. "Sensors are not pliable, and you have to place them more toward the midlines," he said. "You can't place the sensor as easily as the film, but with the Promax you don't even have to think about things like gag reflexes."
More research needed?
But not everyone is convinced that panoramic bitewings are a superior alternative to traditional intraoral bitewings. In a study presented at the 2011 annual meeting of the American Academy of Oral and Maxillofacial Radiology in December, researchers from Ankara University and Gulhane Military Medical Academy compared the two types of images for diagnosing proximal caries and found that intraorals came out ahead.
For this study, they placed 80 extracted human teeth with and without proximal caries in the alveolar sockets of a dry human skull. They obtained intraoral bitewings using Kodak Insight film and extraoral bitewings and panoramic images using the Planmeca Promax system.
The film and printed digital images were evaluated separately by three observers using a five-point scale; evaluations of each image set were repeated one week after the initial viewings. Az values for each image type, observer, and reading were compared using z-tests.
The researchers assessed a total of 160 proximal surfaces of 80 teeth and found that the Az values for both readings of all three observers were highest for the intraoral bitewings. In addition, the Az values for the extraoral bitewing images were higher than those of the panoramic images. No differences (p > 0.05) were found between the Az values of the extraoral bitewing and panoramic images for all observers.
"Intraoral bitewing radiography was superior to extraoral bitewing radiography and panoramic radiography in diagnosing proximal caries of premolar and molar teeth ex vivo," the study authors concluded.
Donald Tyndall, DDS, MSPH, PhD, the director of oral and maxillofacial radiology at the University of North Carolina at Chapel Hill School of Dentistry, also questions some manufacturers' claims.
"Some companies promote pano bitewings for difficult or special cases, such as gagging situations and patients with small mouths, and I'm OK with that," he said. "I am not opposed to the concept of pano bitewings; I just want proof that it works, and we haven't seen that. It is a good concept and worthy of continuing the research. If people have the data [to support pano bitewings], they should publish it in a peer-reviewed journal."