In a series of three articles and videos during February -- Children's Dental Health Month -- DrBicuspid.com is exploring what dental professionals can do to make early childhood visits pleasant and productive for patients and providers alike. Part I focused on the distraction technique. Part II focused on defusing anxiety.
If the ADA has its way, you may soon be seeing babies in your practice, and that could pose some tricky issues. Even a 3-year-old understands "Open your mouth." But what if your patient can't talk?
Since 2001, the American Academy of Pediatric Dentistry (AAPD) has asked caregivers to take their kids to a dentist by the time the child is 1 year old or has a first tooth. The ADA and the American Academy of Pediatrics have signed onto that recommendation as well.
But few dental practitioners ever learned much about examining babies. Why, many ask, should a patient without teeth see a dentist?
|
|
| Leticia Mendoza-Sobel, D.D.S., and Ben Taylor, D.D.S., demonstrate the lap-to-lap technique. |
| Having trouble viewing this clip? Click here to download the free Flash player. |
"It's what pediatricians call 'anticipatory guidance,' " said John Rutkauskas, D.D.S., chief executive officer of the AAPD. "The idea is that we can counsel the caregivers on things they can encounter -- for example, on putting their kids to sleep with a bottle full of a sweet beverage such as orange juice. That's a significant risk factor for caries."
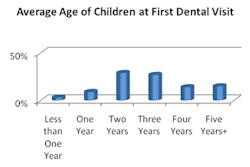
Traditionally, dental guidelines suggested that caregivers take their kids for a first dental visit around age 3. But by age 3, a lot of damage might already have been done.
"A child will often come in at 2 or 2½ years and have a full mouth of decay, and it's just horrible for the practitioner to deal with," said Dr. Rutkauskas.
Not all insurance companies have climbed aboard, but now at least a code is available for making a claim for examining a baby: D0145, Oral Evaluation for a Patient Under Three Years of Age and Counseling With Primary Caregiver.
What to discuss
Some of the topics that dentists should discuss in the first visit include the use of a bottle. Encourage caregivers to give their children liquids, especially juices, in a cup after their first birthday. Children should be weaned from the bottle altogether by 14 months, according to the AAPD. The academy also discourages at-will breastfeeding during the night.
While infants can suck their fingers, caregivers should discourage the habit by the time their kids reach age 4. Also, caregivers should not put honey or any other sweetener on pacifiers.
“A child will often come in at 2 or 2½ years and have a full mouth of decay, and it's just horrible for the practitioner to deal with.”
— John Rutkauskas, D.D.S., CEO,
American Academy of Pediatric
Dentistry
And caregivers should know what to do when their kids' teeth do erupt. Mainly, that means cleaning the teeth, either with a damp washcloth or a small, soft toothbrush, but generally caregivers should not use fluoride toothpaste for children younger than 2, according to the AAPD.
Dental practitioners should also ask the caregivers whether they're giving their kids bottled or tap water, and evaluate whether the tap water contains a sufficient concentration of fluoride. If the child is not getting enough fluoride, practitioners should recommend supplementation, using the AAPD fluoride guidelines.
To help with teething pain, recommend a teething ring (which may or may not be chilled), cool spoon, or cold wet washcloth. Also, caregivers can simply rub the baby's gums with a clean finger.
Finally, caregivers can improve their children's health by attending to their own oral hygiene, both to set a good example and prevent transmission of harmful bacteria. Caregivers should even consider chewing xylitol gum to reduce the spread of caries, according to the AAPD. And they should avoid sharing utensils or cleaning pacifiers with their own mouths.
Lap-to-lap
Of course, that first visit isn't just a discussion time. The practitioner should examine the patient's mouth, looking for any signs of disease or abnormality. But it's hard to do this in a dental chair with very young children.
"Usually they're frightened, so they don't want to sit in the chair," said Leticia Mendoza-Sobel, D.D.S., a Piedmont, CA, pediatric dentist and assistant professor at the University of the Pacific Arthur A. Dugoni School of Dentistry. For these children, she uses the lap-to-lap technique, also known as "knee-to-knee."
The practitioner and caregiver sit facing each other, knee-to-knee. The baby sits on the caregiver's lap, facing the caregiver. The practitioners gently leans the child backward until the child's head is on the practitioner's lap. The caregiver holds the child's hands, while the practitioner examines the child's mouth from an upside-down position.
The child feels the support and guidance of the caregiver, and the practitioner gets better cooperation from the child.
Dr. Mendoza-Sobel recommends the technique for infants and toddlers, preschoolers with behavior problems, and those who are simply too young to mind instructions. It won't stop kids from crying, but usually it keeps the children still enough to allow an examination. And you've got to start somewhere.
Copyright © 2010 DrBicuspid.com