Numb lips, a bitten cheek, slurred words. For years dentists haven't had much choice about causing such temporary discomforts with a nerve block in patients needing mandibular procedures. But recent research suggests an infiltration will suffice for most restorations.
Infiltrations, which target only the nerves of a specific tooth, work just fine in the maxilla. By contrast, the thick bone in the mandible keeps the anesthetic from getting to its target. So the standard recommendation is to use inferior alveolar nerve block (IANB) for any procedures done on the mandible -- much to the distress of many patients. "The thing that makes the patient fearful is that big injection," says Paul A. Moore, D.M.D., Ph.D., M.P.H., chair of dental anesthesiology at the University of Pittsburgh.
In addition to causing less numbness, using infiltration reduces the risk of adverse events associated with IANB, such as trismus, nonsurgical paresthesia, and hemorrhage in hemophiliacs. It's also simpler to master than some of the other alternatives to IANB, such as intraosseous and intraligamentary injections.
The new hope for mandibular infiltrations comes from experiments with articaine, a relatively new local anesthetic that has beaten lidocaine in recent comparative trials. In fact, at the International Association of Dental Research meeting in Toronto in July, Dr. Moore (previously paid as a research consultant for articaine-maker Septodont and other dental supply companies) will present data from a study showing that articaine is more effective than various formulations of lidocaine, prilocaine, mepivacaine, and bupivacaine.
In April 2006, researchers from the University of Newcastle upon Tyne (Journal of Endodontics, April 2006, Vol. 32:4, pp. 296-298) reported some of the first success anesthetizing lower teeth with an articaine infiltration. They were able to numb about 65% of mandibular first molars with articaine, compared to only 39% with lidocaine.
But the study left open the question of how these rates might compare in a matched group of patients getting IANB. Now the same group has reported on such a trial, in the May 2008 Journal of Endodontics (Vol. 34:5, pp. 514-518).
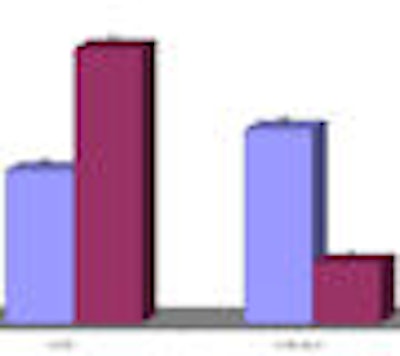
The researchers administered IANB using a solution of 2% lidocaine (1:80,000 epinephrine) to a group of 27 volunteers. Then they zapped the volunteers' first molars with an electronic pulp test. They considered subjects successfully anesthetized if they didn't feel anything at the electrical dose (80 µA) on two consecutive tries. Fifteen of the volunteers (55.6%) achieved that level.
Later, the researchers performed another experiment on the same volunteers, giving them an infiltration of 4% articaine (1:100,000 epinephrine). This time 19 (70.4%) were successfully anesthetized. The difference between the success rate with IANB and rate with infiltration was not significant (p = 0.60).

In the same study, the researchers found that the success rate was equally good whether the volunteers got one buccal infiltration or the same dose of articaine divided evenly between a buccal infiltration and a lingual infiltration.
All but one of the volunteers reported numb lips, but significantly more had numb tongues with the IANB than with the buccal infiltration.
The two-thirds anesthesia success rate might seem small, but the researchers explained that they used a higher standard than would be necessary in the clinic.
"The results presented here provide evidence to support the view that a mandibular infiltration with 4% articaine with epinephrine can be as effective as an inferior alveolar nerve block over the 30-minute study period," the researchers wrote.
So what does that mean to practicing dentists? "I would say most restorative procedures could be done with the infiltration rather than the nerve block," said Sharon Gordon, D.D.S., M.P.H., Ph.D., a professor of biomedical sciences at the University of Maryland. "I myself would probably not try to do a surgical procedure without the nerve block."
Dr. Moore agreed that IANB is still the way to go for the most painful procedures. Citing previous research, he said IANB is effective about 90% of the time, while mandibular infiltration is only effective 60% of the time. He recommended mandibular infiltration for restorations in the incisors and premolars, but not for root canals or extractions and not for extensive restorations in molars. "I think there are many minor procedures where mandibular infiltration is going to work," he said.


















