
Imaging aided in revealing that the rare Eagle syndrome, which is caused by a calcified stylohyoid ligament (SHL), may be linked to dental inflammatory events, specifically root canal treatments, according to a study published on July 26 in the International Dental Journal.
Patients with the syndrome can present with nonspecific difficulty with swallowing, face and neck pain, and dizziness. While Eagle syndrome is not known to cause other medical conditions, the pain can worsen and spread to other body parts if it is not managed or treated.
Cone-beam computed tomography (CBCT) scans showed that root canal treatments were significantly linked to stylohyoid ligament calcification, and the association was independent of other predisposing factors. This is believed to be the first reported study showing an association between SHL calcifications and root canals, the authors wrote.
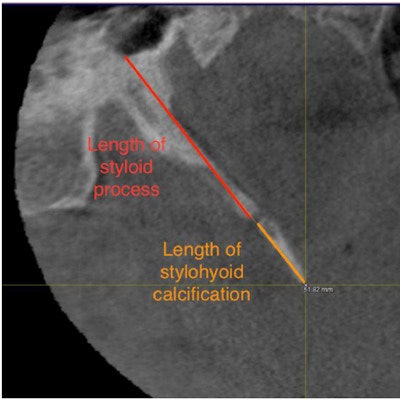
 CBCT in the sagittal plane reveals the length of the styloid process and the length of the stylohyoid ligament calcification. Image courtesy of Al-Amad et al. Licensed by CC BY 4.0.
CBCT in the sagittal plane reveals the length of the styloid process and the length of the stylohyoid ligament calcification. Image courtesy of Al-Amad et al. Licensed by CC BY 4.0."A significant association, however, was found between those calcifications and the number of root canal-treated teeth," wrote the authors, led by Dr. Suhail Al-Amad of the college of dental medicine at the University of Sharjah in the United Arab Emirates.
Eagle syndrome is a rare condition caused by calcification of the SHL. It can occur with or without elongation of the styloid process. Though the cause of calcified SHLs is not fully understood, associations with inflammatory events, including head and neck trauma and tonsillectomy, have been reported.
Since dental diseases occur near SHLs, the authors explored the potential associations between intraoral signs of odontogenic inflammatory events and SHL calcifications. Using CBCT scans from 175 patients, they retrospectively assessed the frequency of dental extractions, root canals, periapical lesions, and furcation lesions, according to the study.
Additionally, the authors gathered information about histories of tonsillectomy and head and neck trauma during phone interviews. They then conducted a logistic regression test to investigate the link between dental events and SHL calcification.
Calcified SHLs were detected on the right side of 71 patients (41%) and the left side of 58 patients (33%). Of patients with SHL calcification, 14% reported having tonsillectomies and 10% reported trauma, the authors wrote.
Among all inflammatory events, root canal treatments correlated significantly with SHL calcification (U value = 2755; standard core [Z] = -2.1; P value = .035). The association was independent of patient age, tonsillectomy, trauma, and other inflammatory events (odds ratio, 1.2; 95% confidence interval, 1.0-1.4; P = .036), the authors wrote.
The study had limitations, including that the correlation between root canals and calcified SHLs were based on imaging occurrence of root canal treatments without measuring the efficacy of those treatments, they wrote. Although the study did not show causal associations between inflammatory events and SHL calcifications, the findings offer a basis to investigate them in the future, the authors wrote.
"Intraoral inflammatory events, particularly related to root canal treatments, have a stronger association with SHL dystrophic calcification than that associated with traditional predisposing factors i.e., old age, tonsillectomy, and trauma," Al-Amad and colleagues concluded.



















